
Electronic Prior Authorization (EPA)
Overview
In recent years, the company has been strategically moving towards a DevOps approach to limit silos and foster communication, automation and continuous delivery of offerings. DevOps, promotes cross functional collaboration between all the parties involved; usually, Dev teams, Business teams, Design teams and other Stakeholders.
To truly take advantage of the DevOps initiative, it was also essential to asses all our product offerings. Most products/features/services are either a result of an acquisitions or built in house, and some even custom code for feature request per customer. This is not ideal for a scalable platform. Thus, our offering were categorized into the buckets below we called Taxanomy.
“Solutions —> Suites —> Products —> Modules —> Features —> services”
Once the Taxanomy was created ,The Change Healthcare Platform (SaaS) allow any healthcare provider to subscribe to parts of a software they need via a Market place. For example, Clinic A might just need to subscribe to a Product with all its modules/features/services (they can turn on/off modules, features and services per their need) while Hospital C might need a Solution for a more robust offering.
It’s at this time, Clearance (conglomerate of products) was broken into different taxonomy groups that can easily be offered via a SaaS offering. As it currently stands, Clearance is an all or nothing offering. A customer would have to purchase it as a whole even if they use a small percentage of what Clearance has to offer.
As the company’s strategies shifted towards a DevOps and SaaS approach, it was decided to rebuild Clearance from ground up.
Electronic Prior Auth (EPA) was one of these taxonomies that needed to be redesigned and rebuilt to
work as a stand-alone application
offered via a marketplace as an add-on with role/org permissions during subscription

A typical Authorization Role and tasks; in some organizations, the Authorization role is coupled with the Eligibility or other front office roles.

This process diagram provides an at-a-glance view of the entire process, helping us visualizes the workflows, the event streams and the API connections that make up the Authorization process. Along with user tasks & workflows involved, this diagram also highlights where possible usability issues may arise.

A swim lane provided by the PMs helps the UX team visualize the structured workflows and various elements of the authorization process. It shows the different steps, indivduals/teams, responsibilities involved but also it illustrates the interaction and collaboration between all parties to achieve a common goal.

These are the step by step task flow of an Authorization role. This task flow helps us ideate and sketch UIs and UX flows

Second One


The goal of this second session was to present our research purpose draft, the draft discussion guide and and discuss through all the information we downloaded from PMs.
Our research purpose is:
To Explore the current process, user interactions between roles and hurdles specific to data gathering during Prior Authorization
In Order To identify areas for improvement in Prior Authorization, data gathering & medical review
So That Change Healthcare can deliver a seamless Authorization and medical review process
In this hour session, we asked the stakeholders “what they want to come back learning?” from this project? We attempted to assess the current state of the Authorization, opportunities for improvement in Prior Authorization & Medical Review along with success metrics and future states of Authorization.
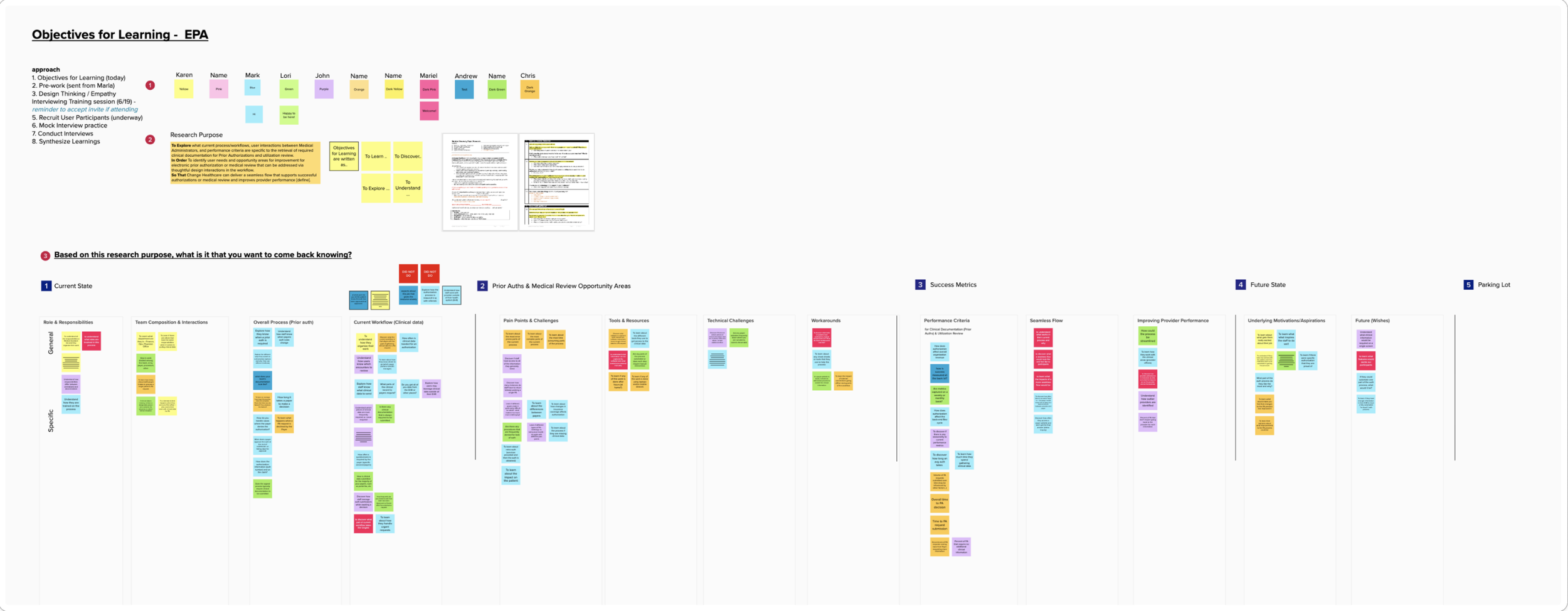
We collected inputs, concerns, ideas and feedback to ensure a collaborative atmosphere. We made sure to capture all that we can from all the stakeholders on the project.
This gives us a working map/direction and ensures everyone is on the same page.

A few insightful stickies pulled from the top board
Make it stand out.
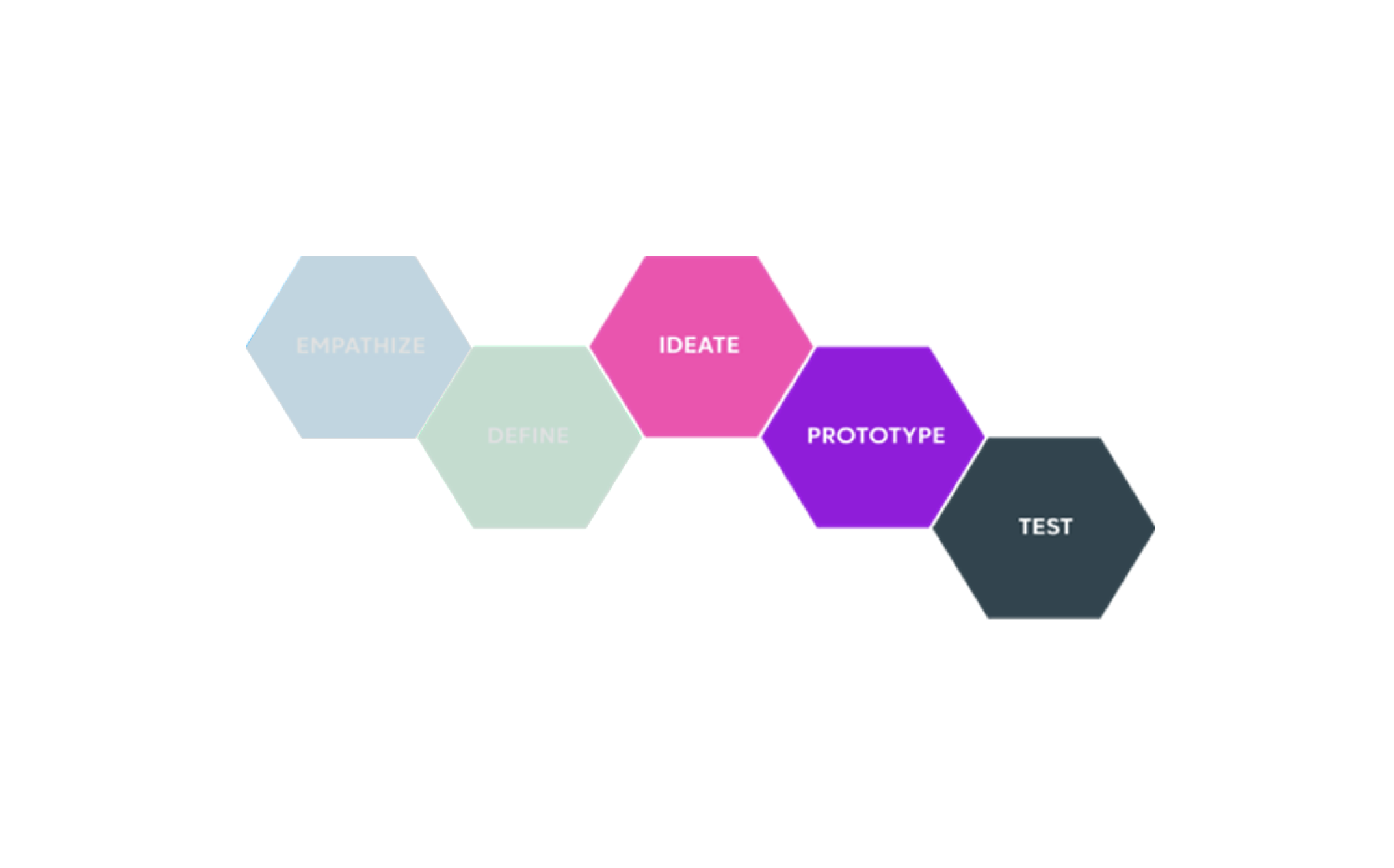
Empathize & Define

Using our design thinking process, we are able to to empathize and define relatively quickly. The kick off meetings offered plenty of knowledge to work from. However, during this phase, we attempt to immerse ourselves in the users’ world; conducting in depth research, interviews, observations etc to truly understand the needs and pain points of our users. This phase is where we come up with a hypothesis or problem statement.
Users almost always will tell you they need everything. There are no substitutions to actually seeing the end user interact with some type of working prototype to observe their behavior and understand the root of their needs and pain points.
We also look into secondary research and similar internal products like Clearance and research rounds from similar products within the organization.
One secondary study we looked at, conducted in 2017 by the American Medical Association, focused on Prior Authorization found -
83% of survey respondents request PA using faxes
63% use a paper form
35% direct through a payer website
14% use an electronic transaction either their EMR or practice management

The problem the business want to solve is clear - business wants to completely digitize the authorization process; and there are countless secondary studies to support it. Usually, in an enterprise level organization, the business sets to solve a clear problem that they know exist. As UX team, we work to validate & solve the problem through thoughtful designs or synthesize a new problem statement supported by research.
The problem statement: As an Authorization Role, I should be able to digitally gather & submit relevant clinical attachments during Prior Authorization for a faster & accurate Authorization approval from payers.
Given what we gathered from PMs and many secondary researches, we opted out of conducting discovery research exclusively but rather we decided to tag on early design concept during the last 15 mins of the 1hr long session. The designs that were used were from a higher taxonomy, Suite Level App called Patient Engagement Suite (PES). The Authorization Module (EPA) would live in PES as permissions allow per Org level subscriptions.

Through these user interviews, we validated the needs and pain points we gathered from PMs and secondary research. Here are a few questions that we asked and the bullet points used to probe further to ensure participants go in detail about the question.
What are your main responsibilities and key areas you support?
What are the most critical aspects of your role or tasks you perform?
What do you spend most of your time on? Why is that?
How are you involved in pulling clinical data for prior authorization with Payers?
What is the most important activity you perform in this process?
How much time per day do you spend on this task?
What determines what clinical data you send?
Where does this data come from? Just EHR or other places?
Are there certain pieces of clinical information that are routinely difficult to obtain, or take additional effort?
Pre Round 2
Make it stand out.
Ideation & Prototyping
Ideation and Prototyping
Using our User Interface Component Library or UICL for short, we can quickly put together concept design for testing. However, before we get to a testing phase we go through iterative design sprints where we meet with the team on a weekly or biweekly basis to get feedback and iterate on designs.
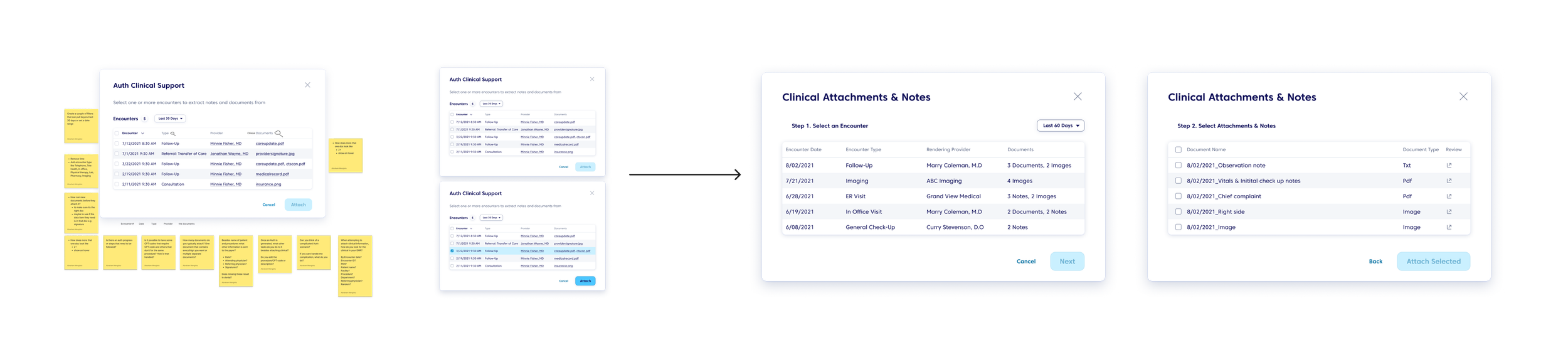
Intitally we started with using Authorizations redesigns I worked on previous to the Taxanomy SaaS approach the company pivoted. The main goal of this round of design and research is to learn more about clinical attachment. How does it work? What are users looking to attach? how do they go about doing that?
Based on what we learned form the discovery potion of our research and secondary research, currently users have to rely on manually scanning documents and either submitting them in the payer portal or faxing documents.
Using previous auth screen design from Clearance that I had previously designed, I started by adding a “attach file” button and using a modal to handle the selection of files.
Over a couple weeks of iteration, we produced the below designs to be tested.

Round 1 of Design after Discovery Research

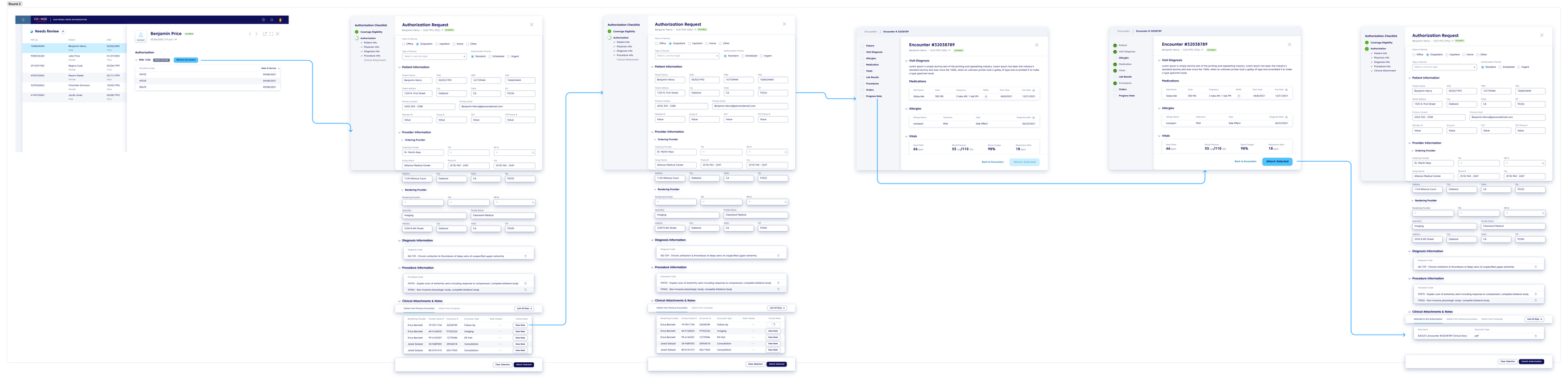
Round 2 of Design





Vivamus pellentesque vitae neque at vestibulum. Donec efficitur mollis dui vel pharetra.